Nasal pathway access
The route begins at the nasal cavity, where olfactory and trigeminal pathways provide direct anatomical connections toward the central nervous system.
A non-invasive pathway for delivering concentrated exosome signaling toward the central nervous system
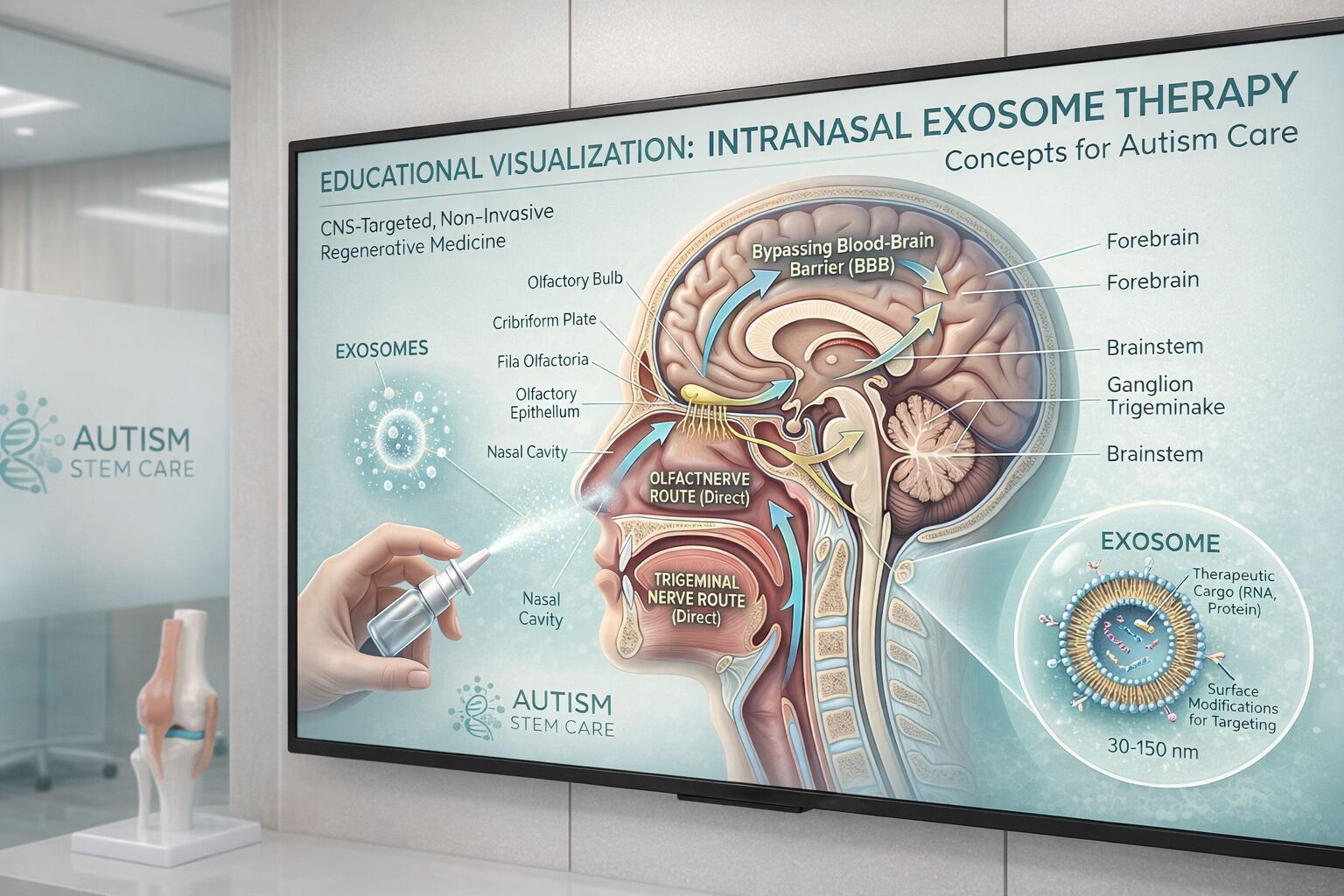
Intranasal administration is an emerging delivery route in regenerative medicine that offers a non-invasive method of introducing MSC-derived exosomes toward the central nervous system. By leveraging the unique anatomy of the nasal cavity — where the olfactory and trigeminal nerve pathways provide direct connections to the brain — intranasal exosome delivery bypasses the blood-brain barrier without the need for lumbar puncture or surgical procedures. Exosomes, as nano-sized extracellular vesicles (30–150 nanometers), are ideally suited for this route due to their small size and ability to travel along neural pathways.
Designed to introduce exosome signaling toward the CNS without lumbar puncture or surgery.
Exosomes are 30–150 nanometers, which makes this route especially relevant for nasal-to-brain transport.
Designed for comfort and minimal invasiveness, making it one of the most child-friendly treatment options available.

The nasal cavity is lined with olfactory epithelium that connects directly to the olfactory bulb in the brain. When MSC-derived exosomes are administered intranasally, their nano-scale size allows them to travel efficiently along the olfactory and trigeminal nerve pathways to reach the central nervous system. This nose-to-brain route allows exosomes to bypass the blood-brain barrier, reach brain tissue through a non-invasive procedure, distribute along neural pathways to areas relevant to neuroinflammation, and deliver concentrated anti-inflammatory microRNAs, proteins, and signaling molecules directly toward the CNS. The procedure involves carefully administering a prepared exosome solution into each nostril using specialized delivery devices while the child is positioned to optimize nasal-to-brain transport.
This delivery route is particularly relevant for families exploring non-invasive CNS-directed options, nose-to-brain therapy, and pediatric alternatives to more invasive delivery methods.

The route begins at the nasal cavity, where olfactory and trigeminal pathways provide direct anatomical connections toward the central nervous system.
Because exosomes are dramatically smaller than whole cells, they are better suited to move through nasal tissues and along neural pathways.
The nose-to-brain route allows targeted signaling to move toward the CNS without requiring lumbar puncture or surgical access.
Exosomes may carry anti-inflammatory microRNAs, proteins, and other signaling molecules toward areas relevant to neuroinflammation and CNS dysfunction.
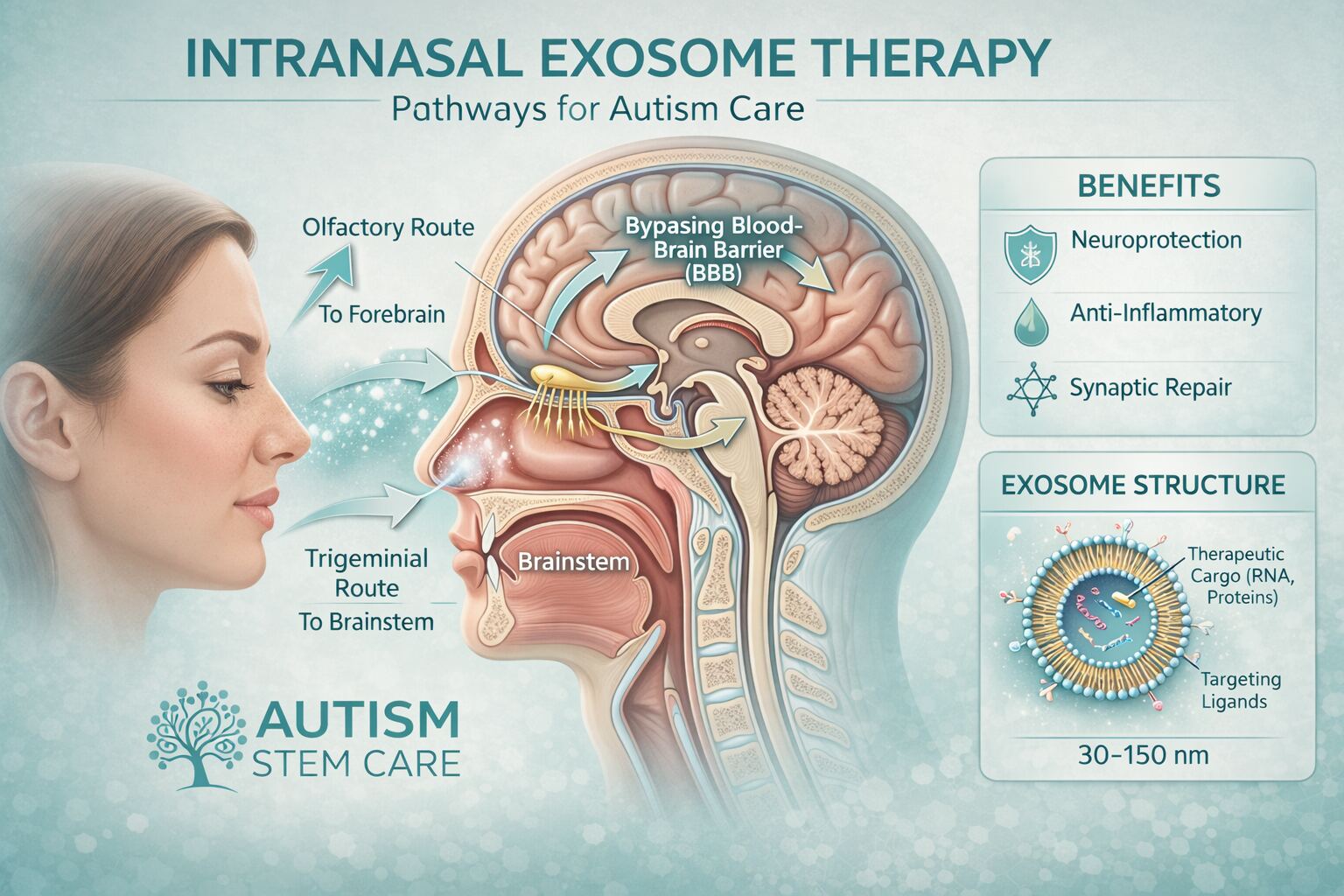
Exosomes are particularly well-suited for the intranasal route because of their nano-scale size — significantly smaller than whole cells. While mesenchymal stem cells are typically 15–30 micrometers in diameter, exosomes are just 30–150 nanometers, allowing them to traverse the nasal epithelium and neural pathways far more efficiently. This means higher concentrations of therapeutic cargo — including anti-inflammatory microRNAs, neuroprotective proteins, and immune-modulating lipids — can reach the brain through this non-invasive route. Exosomes also maintain their biological activity during the transport process, delivering their signaling payload intact to target cells in the CNS.
This delivery pathway is especially attractive for families seeking a central nervous system–directed option without a needle-based spinal procedure.
One of the key practical advantages for families: intranasal exosome delivery can typically be completed comfortably without the need for sedation or anesthesia.
Because exosomes are cell-free, the route avoids the practical burdens associated with live cell administration.
The small size of exosomes is central to why this route is emphasized so strongly in autism-focused regenerative discussions.
Intranasal delivery is often most compelling when paired with systemic or other CNS-directed approaches inside a personalized plan.
The procedure is described as generally well-tolerated and more comfortable than more invasive delivery routes.
For children with autism, intranasal exosome delivery is of particular interest because neuroinflammation and CNS dysfunction are central biological features of the condition. Intranasal exosome administration may support anti-neuroinflammatory effects through direct CNS access, delivery of concentrated neuroprotective and neurotrophic signaling along neural pathways, immune modulation within the brain microenvironment, and complementary support when combined with IV MSC therapy or intrathecal delivery routes. This route is especially appealing for younger children or families seeking less invasive options, as it does not require sedation, anesthesia, or lumbar puncture.
For children with autism, neuroinflammation and CNS dysfunction are central biological features. Intranasal exosome delivery may support anti-neuroinflammatory effects, immune modulation within the brain, and complementary care alongside IV and intrathecal routes. Families researching these options may also want to explore Autism and Neuroinflammation and Autism and Speech Delay.
Our team can help you understand how non-invasive CNS-directed therapy may complement your child's treatment plan.
Intranasal exosome therapy stands out because it combines a CNS-directed rationale with a more comfortable, non-invasive delivery format. For many families, that combination is the reason this page becomes one of the most important treatment pages on the website.
The right way to evaluate it is not in isolation, but within a broader clinical strategy that may also include systemic, intrathecal, or supportive routes depending on the child’s profile.

Intranasal exosome therapy is typically used as one component of a multi-route treatment protocol. It may be combined with intravenous MSC therapy for systemic anti-inflammatory and immune-modulating effects, intrathecal MSC administration for direct cerebrospinal fluid delivery when clinically indicated, IV exosome therapy for systemic cell-free signaling, and supportive IV nutrient therapies. Our medical team determines whether intranasal exosome delivery is appropriate for each child based on their clinical profile, age, and treatment goals during the personalized treatment planning process.
Learn about exosome therapy as a standalone treatment and understand the broader role of cell-free signaling in autism-focused regenerative medicine.
Visit treatment pageCompare non-invasive intranasal delivery with direct cerebrospinal fluid administration to understand which CNS-directed route may be most appropriate.
Visit treatment pageLearn how systemic IV stem cell therapy may complement intranasal exosome delivery within a multi-route treatment protocol.
Visit treatment pageExplore how intranasal, intravenous, intrathecal, and supportive therapies can be combined in comprehensive multi-route protocols.
Visit treatment pageIntranasal exosome administration is generally well-tolerated. The procedure is non-invasive, does not require sedation, and can typically be completed in a comfortable clinical setting. Because exosomes are cell-free, they carry no risk associated with live cell administration. Some children may experience mild, temporary nasal irritation. As with all treatment modalities, our medical team discusses potential benefits, limitations, and risks transparently with families before including intranasal delivery in any treatment protocol.

Understand why neuroinflammation is a key treatment target in autism and how CNS-directed approaches may help address it.
Explore conditionLearn about autism spectrum disorder and the biological factors that make regenerative medicine approaches relevant for some children.
Explore conditionUnderstand the connection between autism and speech delay, and how neurological support may be relevant for language development.
Explore conditionAnswers to the most common questions families ask when exploring intranasal exosome delivery for their child.
Intranasal exosome delivery is non-invasive and generally well-tolerated. The procedure involves administering a solution into the nostrils — similar to nasal spray — and does not require needles, sedation, or anesthesia. Some children may experience mild, temporary nasal discomfort.
Exosomes are nano-sized vesicles (30–150 nanometers) — far smaller than whole mesenchymal stem cells (15–30 micrometers). This tiny size allows exosomes to traverse the nasal epithelium and neural pathways much more efficiently, delivering concentrated therapeutic cargo directly toward the brain. Exosomes are also cell-free, which simplifies the administration process.
Both routes aim to deliver therapeutic agents toward the CNS. Intrathecal delivery places MSCs directly into the cerebrospinal fluid via lumbar puncture and may achieve higher local concentrations. Intranasal exosome delivery is non-invasive and uses neural pathways to reach the brain. Our medical team may recommend one or both routes depending on the child's clinical needs.
While intranasal exosome therapy can be administered independently, it is most commonly included as part of a multi-route protocol that may also involve IV MSC therapy and/or intrathecal delivery. The optimal approach is determined during personalized treatment planning.
Our medical coordination team can discuss your child's unique needs, explain the role of intranasal delivery within a broader treatment framework, and help you understand whether this non-invasive approach may be appropriate. Free, no-obligation consultation.
Free medical review
Personalized guidance for your child